

























Varicose veins most often affect the venous system of the legs. External manifestations (protruding nodular blue veins, swelling) are not just a cosmetic problem, but signs of a serious disease that worsens over time.
What are varicose veins: definition of the disease
The word "varicose veins" comes from the Latin varix - "swelling". The name fully reflects the pathological process: the walls of the veins become thinner, and in some areas expansions (sac swelling) - nodes are formed.
The first case of varicose veins was recorded in a document from 86 BC. C. a. C. : the Roman general Gaius Marius complained of pain in his legs due to "swollen blue veins".
The main reason for the development of varicose veins (varicose veins, varicose veins) is an increase in pressure in the system of superficial vessels. This is facilitated by certain diseases, hormonal changes and a sedentary lifestyle.
Initially, even under the influence of these factors, the vessels function normally, but gradually they deform, change their structure and can no longer fully transport blood.
Varicose veins can develop in almost any part of the body, but most often appear in the lower extremities. Therefore, when we talk about varicose veins, by default we mean the problem of the legs.
Code for varicose veins in ICD-10
The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) includes several types of varicose veins.
I83 - varicose veins of the lower extremities:
- I83. 0 - varicose veins of the lower extremities with ulcers;
- I83. 1 - varicose veins of the lower extremities with inflammation;
- I83. 2 - varicose veins of the lower extremities with ulcers and inflammation.
85 - varicose veins of the esophagus:
- I85. 0 - varicose veins of the esophagus with bleeding;
- I85. 9 - varicose veins of the esophagus without bleeding.
I86 - varicose veins of other localizations:
- I86. 0 - varicose veins of the sublingual veins;
- I86. 1 - varicose veins of the scrotum (anatomical formation in men - a receptacle for the testicles and their appendages);
- I86. 2 - varicose veins of the pelvis;
- I86. 3 - varicose veins of the vulva (external genitalia of a woman);
- I86. 4 - varicose veins of the stomach.
O22. 0 - varicose veins of the lower extremities during pregnancy.
In our country 30 million people suffer from various forms of varicose veins. A third of them have complications: trophic ulcers. An open defect in the skin or mucosa that occurs due to impaired blood circulation and tissue innervation.
The mechanism of development of varicose veins
The pathological reactions of the body are the same for all types of varicose veins, regardless of the cause of the problem. Understanding the anatomical characteristics of blood vessels will help understand how and why the disease develops.
How blood moves through the body
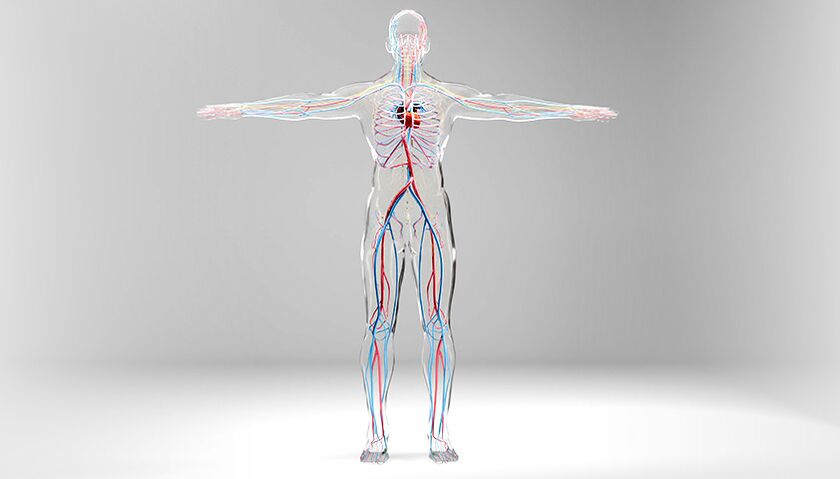
There are two types of vessels in the human body: veins and arteries. Blood flows through arteries from the heart to all organs and tissues. This occurs at high pressure (70–120 mm Hg) and high speed.
Blood flows through the veins from organs and tissues, is directed to the heart at low pressure (0–20 mm Hg).
The walls of veins are less thick and elastic than the walls of arteries and, unlike arteries, do not contain such a developed muscle layer. Therefore, varicose veins are possible only in veins, but not in arteries.
Human arterial and venous circulatory system. Veins are indicated in blue, arteries in red.
Low pressure in the veins is necessary to transport blood from the periphery to the center. But at the same time, on the way to the heart, blood flow encounters an obstacle - the force of gravity. This force forces the blood back through the veins.
We often hear that varicose veins are humanity's punishment for walking upright. After all, the longest distance blood has to travel in the body, overcoming gravity, is the path from the feet to the heart. The movement of blood through the veins is ensured by contractions of the heart, the muscle pump of the surrounding muscles and the negative pressure in the chest during inspiration.
In healthy vessels, the reverse flow of blood is prevented by valves located on the internal walls of the veins. The valves act like one-way swing doors: They open and allow blood to flow to the heart, and close immediately if gravity tries to push the blood back.
It is not only the valves that help the veins carry blood to the heart, but also the muscles that surround the vessels. By contracting and relaxing, muscles help move blood through the veins. This mechanism works only when a person moves. When you stand or sit for a long time, the muscle pump is practically inactive.
The cusps of the venous valves always face in the direction of blood flow, towards the heart
How failure occurs and disease occurs
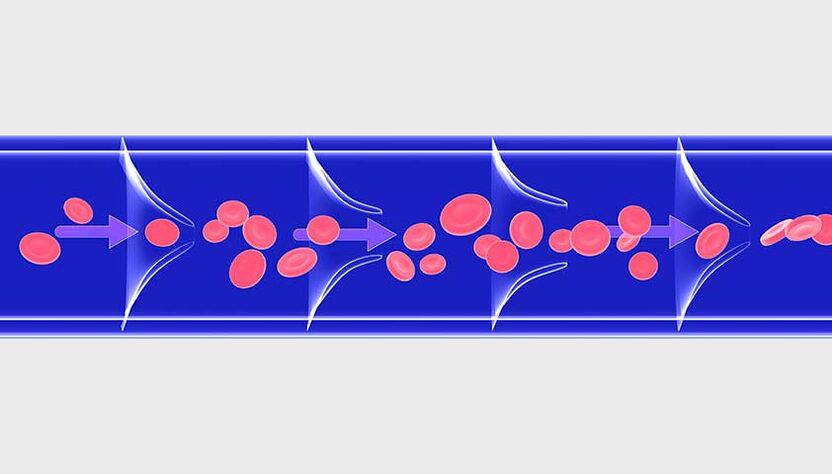
An increase in pressure in the venous system disrupts the functioning of their valve apparatus and leads to the reversal of blood flow through the vessels. For this reason, as well as due to stagnation of excess blood, weakness of the valve apparatus (for example, in connective tissue diseases), the lumen of the veins expands, the walls are deformed, become thinner and similar local protrusions - knots are formed in pockets.
The process is similar to inflating a balloon: if you don't let the air out, the balloon inflates more and more.
On the left is normal blood flow; on the right - multidirectional blood flow due to impaired functioning of venous valves, vascular deformation

In the legs there are superficial and deep veins. 85-90% of the total blood volume passes through the deep ones, only 10-15% through the superficial ones. The walls of the deep veins are denser and better suited to increasing blood volume. And the superficial veins of the legs are thinner and more susceptible to varicose veins.
In the pelvis and lower parts of the esophagus there are large venous plexuses, which can also undergo varicose transformation. In the veins of the small pelvis, the mechanism of development of the disease is the same as in the lower extremities. But varicose veins of the esophagus arise for another reason: due to portal hypertension - increased pressure in the portal venous system, which develops with liver cirrhosis, hepatitis, parasitic liver lesions, fatty hepatosis, etc.
Causes of varicose veins
Numerous factors contribute to the development of varicose veins in the legs. The main ones arevalvular insufficiencyANDinheritance. It is known that a quarter of patients had close relatives suffering from one of the forms of varicose veins.
Overweight. The more extra kilos a person has, the greater the load on the venous system. Over time, the veins cease to cope with such pressure: the lumen of the vessels increases, and the valves on their walls cease to close completely. As a result, blood stagnation occurs and varicose veins develop.
Pregnancy. Hormonal changes occur in a woman's body, body weight, intra-abdominal pressure and increased volume of circulating blood - this leads to disruption of outflow, causes stretching of the walls of veins and changes in functioning of the valvular system.
After childbirth, the diameter of the dilated veins decreases, but does not always return to the original value. With subsequent pregnancies the risk of developing varicose veins increases.
Age. Varicose veins often affect people after the age of 50. The older a person is, the more the venous valves wear out, the recovery processes slow down and the mechanism of pathological expansion of the veins is activated - the development of varicose veins.
Venous refluxVenous refluxReturn of blood through the veins due to resistance to blood flow, from Lat. refluo – "to flow backwards". found in 10-15% of schoolchildren aged between 12 and 13. The disease "rejuvenates" due to a sedentary lifestyle and excess weight.
Varicose veins of the lower extremities develop more quickly if additional risk factors are present.
Risk factors that contribute to the development of varicose veins in the legs:
- lack of physical activity: during movement, muscles stimulate blood flow in the veins, and without movement, blood circulation in the veins may be difficult;
- smoking: chemicals contained in tobacco smoke damage the walls of blood vessels, as a result their lumen narrows, blood flow becomes difficult and stagnation occurs, which leads to varicose veins;
- professions that require standing or sitting for long periods of time are at risk: hairdressers, surgeons, cooks, waiters, drivers, clerks;
- menopause - in women aged 40-50 years, the production of sexual hormones (estrogen and progesterone) decreases and at the same time the tone of the venous wall decreases. This increases the chance of varicose veins.
Women suffer from varicose veins 3-4 times more often than men. This occurs due to hormonal variability (menstrual cycle, pregnancy, menopause).
During pregnancy, varicose veins can affect different parts of the body: legs, thighs, vulva

Varicose veins can occur not only in the lower extremities, but also in other parts of the body.
The main causes of varicose veins in various locations
Varicose veins of the esophagus
Changes in the veins of the esophagus with uneven increase in their lumen, protrusion of the wall and development of nodular tortuosity of the vessels. It often leads to a life-threatening complication: bleeding.
Reasons:
- cirrhosis
- liver cancer
- other diseases that cause increased pressure in the portal vein system: it collects blood from the abdominal organs
Varicose veins of the scrotum (varicocele)Pathological dilation of the veins of the pampiniform plexus of the testicle. Manifested by varicose veins in the scrotum and impaired blood flow
Reasons:
- congenital incompetence of the valves of the testicular veins (usually the left one)
- mechanical compression of the testicular vein (inguinal hernia)
Varicose veins of the pelvis
It is characterized by dilation of the ovarian veins and intrapelvic venous plexuses of various diameters. The condition is also known as pelvic congestion syndrome
Reasons:
- polycystic ovary syndrome
- two or more pregnancies
- hormonal dysfunction
Varicose veins of the vulva
Varicose veins of the pelvis, which affect the vessels of the labia and perineum
Reasons:
- compression of the retroperitoneal vessels by the uterus during pregnancy
- significant physical activity
- tumors of the uterus and ovaries
Varicose veins of the sublingual veins (sublingual varicose veins)
Asymptomatic damage to the veins located under the tongue. It manifests itself as a slight protrusion of blood vessels and a color change from deep blue to purple
Reasons:
- hypertension
- smoking
- old age
Varicose veins of the stomach
Isolated change in the veins of the stomach or combined with varicose veins of the esophagus
Reasons:
- cirrhosis
- portal hypertension syndrome - increased pressure in the portal venous system in other gastrointestinal diseases (neoplastic tumors, thrombosis, anomalies of venous development)
Symptoms of varicose veins
In rare cases, only the cosmetic side of the disease appears: bluish veins. Most patients suffering from varicose veins of the legs report at least one or more unpleasant symptoms.
Symptoms of varicose veins of the lower extremities:
- fatigue, pain or feeling of heaviness in the legs - this is caused by blood stagnation and its pressure on surrounding tissues;
- burning, tingling or throbbing in the legs - a reaction to slowing blood flow and overflowing the venous system of the lower extremities;
- nocturnal muscle cramps in the legs: painful spasms occur due to blood stagnation and the accumulation of metabolic products in the tissues;
- swelling of the feet and ankles - due to stagnation in the veins, the liquid part of the blood penetrates into the subcutaneous tissue through the altered vascular wall;
- itchy skin around damaged veins - dilated and impaired blood vessels do not provide normal blood circulation and nourishment to the skin, so it becomes dry and rough.
Unpleasant sensations in the legs in patients with varicose veins intensify in the evening, especially after long periods of sitting or standing.
The appearance of altered veins is not always proportional to the severity of the symptoms. Therefore, veins that are barely visible to the eye and affected by varicose veins can cause severe discomfort, while nodular and thickened veins can cause minimal concern.

Varicose veins affect different veins: from small vessels in the skin to large saphenous veins
Symptoms of other types of varicose veins largely depend on the underlying cause of the disease. Often patients do not complain about anything, and the doctor identifies the problem only during the examination. This happens, for example, with varicose veins of the sublingual veins.
In some cases, as in the case of varicose veins of the esophagus or stomach, the pathology immediately manifests itself as a life-threatening complication: bleeding.
Classification of venous diseases
In clinical practice, doctors rely on the international classification of venous diseases - CEAP. This is an abbreviation formed from the initial letters of the main sections of the classification:
- C — clinical (clinical changes);
- E — etiology (origin of the disease);
- A - anatomy (anatomical localization of varicose veins);
- P - pathogenesis (mechanism of venous blood flow disorders).
Complications of varicose veins on the legs
Typically, varicose veins themselves are not life-threatening. But sometimes the disease can cause complications.
Thrombophlebitis- inflammation of the walls of the veins, which is accompanied by the formation of a thrombus (blood clot) that closes the lumen of the vessel. It manifests as swelling and redness along the affected vein. The patient feels pain, the skin in the affected area becomes red and hot to the touch.

Thrombophlebitis is an inflammatory reaction of the skin and subcutaneous tissue along the course of a thrombosed vein.
Venous trophic ulcer- an open defect of the skin and soft tissues due to blood stagnation, edema and impaired cellular nutrition. The ulcer occurs on the legs and ankles near the areas of varicose veins. In the lower parts of the legs the swelling is more pronounced, which means that the tissues are compressed more than in other areas. Ulcers take a long time to heal and often contain bacteria that increase inflammation.
Trophic ulcers heal very poorly due to impaired blood circulation and tissue nutrition

Bleeding- occurs when a vein ruptures, dilated due to varicose veins. In the later stages of the disease, the skin over these veins is very thin and dry: a slight injury is enough to compromise the integrity of the vessel and cause bleeding. Sometimes a spontaneous rupture of a vein occurs in the area of varicose nodes.
Diagnosis of varicose veins of the legs
The phlebologist deals with the diagnosis, treatment and prevention of venous diseases. The doctor makes a diagnosis based on the patient's complaints, examination and instrumental studies. If the symptoms of varicose veins are pronounced, tests are usually not prescribed - a medical examination is enough.
The doctor may prescribe laboratory tests in preparation for surgery or to exclude concomitant diseases that affect the condition of the blood vessels.
One of these diseases is diabetes mellitus. It can significantly worsen the course of varicose veins and increase the risk of complications (especially trophic ulcers).
For an accurate diagnosis and determination of treatment tactics, duplex ultrasound scanning, the gold standard for diagnosing vascular conditions, will be necessary. The method allows you to evaluate the structure, function, patency of superficial and deep veins, the consistency of valves, and also to determine the direction of blood flow.
If a secondary nature of varicose veins is suspected (can occur after deep vein thrombosis), the doctor prescribes venography, CT venography or MRI.
Phlebography is an x-ray test used to determine the patency of the deep veins and valve function.
Computerized or magnetic resonance venography is used to visualize the venous system in three-dimensional projection and with a very high spatial resolution.
Treatment of varicose veins on the legs
The goal of treating varicose veins is to reduce or eliminate symptoms, improve the appearance of the veins, and prevent complications.
The doctor chooses a treatment method depending on the affected vessels and the severity of the patient's condition with varicose veins.
Non-invasive treatments
Noninvasive treatments for varicose veins include compression therapy, drug therapy, and lifestyle changes.
Compression therapy involves the use of socks, hold-ups and special pantyhose. The choice of model, type of fabric and degree of compression depends on the symptoms. The doctor will help you choose the appropriate hosiery.
The compression shirt in the lower legs compresses more than in the upper legs, thus pushing the blood towards the heart and eliminating stagnation

Effects of compression therapy for varicose veins:
- symptom manifestations decrease: heaviness, leg fatigue, night cramps, burning sensation or pain;
- the severity of edema is reduced due to improved blood circulation;
- Healing of trophic ulcers is accelerated, because elastic compression improves blood circulation and tissue nutrition.
Drug therapy - the doctor may prescribe phlebotropics Phlebotropic drugs (phleboprotectors, venotonics) Biologically active substances that increase venous tone and reduce the severity of venospecific symptoms. drugs (venotropics).
The main groups of phlebotropic drugs used for varicose veins:
- angioprotectors: improve microcirculation, normalize the increase in capillary permeability, reduce blood viscosity and the likelihood of blood clots;
- antithrombotic agents: they reduce the risk of the formation of dangerous blood clots (thrombi) in the lumen of blood vessels and promote the dissolution of existing ones;
- bioflavonoids: natural plant compounds that improve venous tone and reduce venous congestion.
Lifestyle changes for varicose veins significantly slow down the development of the disease and, in combination with other recommendations of the attending physician, help to stop the pathological process.
Important indications for changing the lifestyle of patients with varicose veins:
- moderate intensity exercises: walking, swimming, water aerobics, leg exercises, yoga. Strengthening the muscles will help normalize blood circulation in the vessels, relieve venous stagnation and edema;
- weight control: thanks to the normalization of body weight, the load on the blood vessels is reduced and the return of blood through the veins to the heart is facilitated;
- abandon bad habits: nicotine and alcohol damage the internal walls of blood vessels and disrupt the regulation of vascular tone. Quitting smoking and drinking alcohol improves the condition of the veins and the function of the valves.
Invasive methods for the treatment of varicose veins
Invasive treatments include medical procedures that compromise the integrity of the skin or mucous membranes. Sclerotherapy is a procedure that uses a special sclerosing (sclerosing) solution. The solution is injected into the problem vein through a thin needle, which causes its sclerosis - "gluing". The vein is quenched by blood flow and over time becomes invisible; its function is taken over by nearby veins. Sclerotherapy is performed without hospitalization: after the procedure the patient can return home.
The sclerotherapy procedure lasts from 5 to 30 minutes, depending on how many varicose veins need to be filled with sclerosant and how large they are

Endovenous laser thermoobliteration (EVLO). A catheter with a laser light guide is inserted into the vessel through a small incision. The thermal energy of the laser heats the vein and it is obliterated: "sealed". After a few months, the vessel is replaced by connective tissue and disappears. The procedure is performed on an outpatient basis.
Radiofrequency vein obliteration (RFO) is the effect of high-frequency current on the inner surface of blood vessels. Through a micropuncture, a catheter connected to a device that generates radiofrequency pulses is inserted into the vein. Inside the vessel, the radio wave is converted into thermal energy, which "seals" the vein.
With EVLO the vein is briefly exposed to a high temperature; with RFO the temperature is lower, but the session is longer. Both procedures are effective and safe.
NTNT obliteration or non-thermal and non-tumescent methods:
- venous obliteration using cyanoacrylate glue;
- mechanochemical obliteration, in which mechanical and chemical effects on the vessel occur simultaneously.
Obliteration of the NTNT is the most modern and least traumatic method of treating varicose veins with a short rehabilitation period.
Phlebectomy is the removal of saphenous veins that have suffered from varicose veins. It can be performed as an independent operation or combined with other techniques. The varicose vein is removed under local anesthesia through small punctures.
Prevention of varicose veins of the legs
It is possible to prevent the development of varicose veins if you follow simple prevention rules in everyday life.
A combination of provoking factors – sitting for long periods of time with legs crossed, wearing uncomfortable shoes – increases the risk of varicose veins in the legs.

Prevention of varicose veins: what you need to know:
- moderate physical activity (walking, swimming, leg exercises) and rest with raised legs improves free circulation of blood through the vessels and helps avoid stagnation in the veins;
- rational nutrition and weight normalization lead to the strengthening of blood vessels;
- wearing loose clothing that does not restrict movement helps improve blood circulation;
- a cool shower in hot weather helps keep veins toned;
- comfortable shoes with low heels (no more than 3 cm) allow you to avoid improper load on the foot and disruption of blood flow;
- A reasonable approach to visiting saunas and steam rooms allows you to maintain normal blood flow (long-term thermal procedures significantly dilate the veins, so blood flow slows down).